2009 H1N1 and Seasonal Influenza Infections and Invasive Pneumococcal Disease
Some of CDC's Active Bacterial Core surveillance (ABCs) sites have seen an increase in serious cases of pneumococcal disease coincident with increases in influenza-associated hospitalizations. CDC has been working with state and local public health officials in Colorado for example concerning its ABCs site in the Denver Metro area to collect additional data on pneumococcal disease cases.
There is good evidence that 2009 H1N1 influenza may be responsible for this increase in invasive pneumococcal disease (IPD) cases in the Denver Metro area. (5-year average number of cases in October, ~20; total number in October 2009, 58).
The increase in IPD cases in the Denver Metro area is primarily among younger adults with 36 out of 58 (62%) cases occurred among 20-59 year olds. In a typical non-pandemic year, most IPD cases occur among persons 65 years of age and older.
What occurred in Denver is likely an indicator of what is happening in other parts of the country. Data shown below is preliminary and subject to change upon further investigation.
For more information on preventing pneumococcal infections secondary to seasonal and 2009 H1N1 influenza: http://www.cdc.gov/h1n1flu/vaccination/public/public_pneumococcal.htm.
2009 H1N1 Influenza Vaccination Safety
How many adverse event reports among people who received 2009 H1N1 vaccine have been reported to CDC?
As of November 20, 2009, the CDC Vaccine Adverse Event Reporting System (VAERS) had received 3,182 adverse event reports following 2009 monovalent H1N1 vaccination. The vast majority (94%) of adverse events reported to VAERS after receiving the 2009 monovalent H1N1 vaccine have not been serious (e.g., they encompass things like soreness at the vaccine injection site). CDC and FDA will be providing weekly updates on our vaccine safety monitoring activities in an effort to better characterize data that are being viewed publicly through the Vaccine Adverse Event Reporting System (VAERS;
and CDC’s website, WONDER (
http://wonder.cdc.gov/vaers.html).
How does 2009 H1N1 vaccine safety compare to seasonal flu vaccine safety?
The number of serious health events reported after H1N1 vaccination is very similar to the number of reports that typically follow seasonal influenza vaccines. Additionally, no new or unusual events or pattern of adverse events have emerged.
How many Guillain-Barré syndrome (GBS) cases have been reported after 2009 H1N1 vaccination?
We know there has been interest in Guillain-Barré syndrome (GBS). CDC employs three vaccine monitoring systems that will alert us quickly should any indications of GBS-related issues arise, including: Vaccine Adverse Event Reporting System (VAERS), Vaccine Safety Datalink (VSD), and a collaboration in 10 states to look actively look for cases of GBS regardless of vaccination. To date, there are no indications of GBS-related problems with the 2009 H1N1 vaccine. It is important to note that each week in the United States, about 80-160 cases of GBS occur in the general population - regardless of vaccination. For more information about GBS:
http://www.cdc.gov/h1n1flu/vaccination/factsheet_gbs.htm.
How is the government monitoring H1N1 vaccine safety?
The Federal government has a robust vaccine safety monitoring program that has been enhanced further to ensure 2009 H1N1 vaccine safety.
Reports of Changes to the 2009 H1N1 Virus
November 24, 2009 6:00 PM ET
Have changes to the 2009 H1N1 virus been reported?
The majority of 2009 H1N1 viruses tested by CDC and the other three World Health Organization (WHO) Collaborating Centres located around the world are similar and have changed relatively little since April 2009 when the 2009 H1N1 virus was first detected. However, there have been occasional reports of small changes in the genes of some virus samples collected from some people infected with 2009 H1N1 in several countries.
What are these changes to the 2009 H1N1 virus and what are the implications for public health?
The changes to the 2009 H1N1 virus that have been
reported out of Norway, and that
WHO has reported as being detected occasionally in viral isolates in other countries, are scientifically known as D222G and D222N changes. The public health implications of these changes are currently being studied by CDC and WHO scientists. At this time, these changes appear to occur sporadically and spontaneously. No links between the small number of patients infected with 2009 H1N1 virus with these changes have been found, and viruses with these changes do not appear to be spreading to other people. Although further investigation is underway, there is no evidence that these changes in the 2009 H1N1 virus have lead to an unusual increase in the number of 2009 H1N1 infections or to a greater number of severe or fatal cases. Worldwide, these changes have been found in mild cases of 2009 H1N1 illness as well as severe cases of illness that have resulted in death. As a result, the public health significance of this finding remains unclear.
Will the 2009 H1N1 vaccine still protect against these viruses?
According to CDC and WHO experts, the 2009 H1N1 vaccine remains well matched with the 2009 H1N1 viruses that contain these small changes. There is no reason to think that the 2009 H1N1 vaccine will be less effective against these viruses based on the area of the influenza virus where these changes have occurred.
Will antiviral drugs work against the 2009 H1N1 viruses that have these changes?
The D222G and D222N changes found in these 2009 H1N1 isolates are not associated with resistance to oseltamivir or any other influenza antiviral medication.
Which countries have reported finding 2009 H1N1 viruses with these changes?
A recent report from the Norwegian Institute of Public Health described a change in the 2009 H1N1 virus (D222G) found in the first two people in Norway who died from 2009 H1N1 as well as an additional Norwegian patient with severe influenza illness. This D222G change was not found in the virus samples isolated from other people who died in Norway of 2009 H1N1 related causes. Norwegian scientists have analyzed samples from more than 70 patients infected with 2009 H1N1, and no additional viral isolates containing these changes have been found.
In addition to Norway, CDC has received sporadic reports of these changes found in viral isolates from Australia, Brazil, China, Japan, Mexico, Saudi Arabia, Ukraine, Uruguay and the United States.
2009 H1N1 Hospitalizations in People with Asthma November 4, 2009
What does CDC know about hospitalizations among people with asthma who get 2009 H1N1 flu?
People with asthma are at higher risk for serious complications from influenza (flu), including 2009 H1N1 flu. This can place people with asthma at higher risk of hospitalization when they have 2009 H1N1 flu. CDC monitors 2009-H1N1 related hospitalizations, including among people with asthma, through the Emerging Infections Program (EIP).
What is the Emerging Infections Program (EIP)?
The EIP Influenza Project conducts surveillance for laboratory-confirmed influenza (flu) related hospitalizations in children (persons younger than 18 years) and adults in 62 counties covering 13 metropolitan areas of 10 states (for more information see the overview of influenza surveillance in the United States). Cases are identified by reviewing hospital laboratory and admission databases and infection control logs for children and adults with a documented positive influenza test* conducted as a part of routine patient care. EIP estimated hospitalization rates are reported every week during the flu season.
*Tests used by EIP to confirm influenza infection include viral culture, direct/indirect fluorescent antibody assay (DFA/IFA), real-time reverse transcriptase polymerase chain reaction (rRT-PCR), or a commercial rapid antigen test.
What percentage of people hospitalized with 2009 H1N1 flu have asthma?
According to Emerging Infections Program (EIP) data collected from April 15 through October 27, 2009, 32% of people hospitalized with 2009 H1N1 had asthma. Among adults hospitalized with 2009 H1N1, 30% had asthma, whereas 35% of hospitalized children with 2009 H1N1 had asthma.
What percentage of people hospitalized with asthma and 2009 H1N1 are admitted to an Intensive Care Unit (ICU)?
According to Emerging Infections Program (EIP) data collected from April 15 - October 27, 2009, 21% of hospitalized adults with asthma and a 2009 H1N1 infection and 18% of hospitalized children with asthma and a 2009 H1N1 infection were admitted to an ICU. No significant differences in the number of ICU admissions were noted between 2009 H1N1 infected people hospitalized with or without asthma.
2009 H1N1 Hospitalizations by Age Group
October 20, 2009 What percentage of hospitalizations for 2009 H1N1 flu occur in different age groups in the United States?
The percentage of hospitalizations for 2009 H1N1 flu in the United States varies by age group. From August 30, 2009 through October 10, 2009, states reported 4,958 laboratory-confirmed 2009 H1N1 hospitalizations to CDC. The percentage of 2009 H1N1 related hospitalizations that occurred among those 0 to 4 years old was 19%; among those 5 years to 18 years was 25%; among people 19 years to 24 years was 9%; among those 25 years to 49 years was 24%; among people 50 to 64 years was 15%; and among people 65 years and older was 7%. For a graphical representation of this data, please see the chart below.
 What percentage of deaths for 2009 H1N1 flu occur in different age groups in the United States?
What percentage of deaths for 2009 H1N1 flu occur in different age groups in the United States?
The percentage of deaths for 2009 H1N1 flu in the United States varies by age group. From August 30, 2009 through October 10, 2009, states reported 292 laboratory-confirmed 2009 H1N1 deaths to CDC. The percentage of 2009 H1N1 related deaths that occurred among people 0 years to 4 years was 3%; among those 5 years to 18 years was 14%; among people 19 to 24 years was 7%; among people 25 to 49 years was 33%; among people 50-64 years was 32%; and among people 65 years and older was 12%. For a graphical representation of this data, please see the chart below.
















 Download 72 dpi JPEG image:
Download 72 dpi JPEG image: Download 72 dpi JPEG image:
Download 72 dpi JPEG image: Download 72 dpi JPEG image:
Download 72 dpi JPEG image:


 Download 72 dpi JPEG image:
Download 72 dpi JPEG image: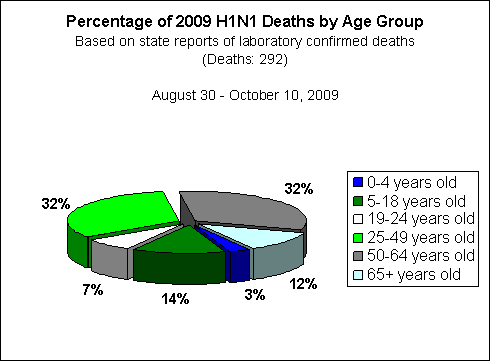
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}